
Dynomight
Acetaminophen, ibuprofen, and what doctors probably want you to know.
Lots of people die after overdosing on acetaminophen (paracetamol, often sold as Tylenol or Panadol). In the U.S., it’s estimated to cause 56,000 emergency department visits, 2,600 hospitalizations, and 500 deaths per year. Acetaminophen has a scarily narrow therapeutic window. The instructions on the package say it's okay to take up to four grams per day. If you take eight grams, your liver could fail and you could die.
Meanwhile, it seems to be really hard to kill yourself by overdosing on ibuprofen (Advil, Nurofen, Motrin, Brufen). In 2006, Wood et al. searched the medical literature and found 10 documented cases in history. Nine of those cases involved complicating factors, and in the 10th, a woman took the equivalent of more than 500 standard (200mg) pills.
So, for many years, if I needed a painkiller, I’d try to take ibuprofen rather than acetaminophen. My logic was that if eight grams of acetaminophen could kill my liver, then one gram was probably still hard on it. I’m fond of my liver and didn't want to cause it any unnecessary inconvenience.
But guess what? My logic was wrong and what I was doing was stupid. I’m now convinced that for most people in most circumstances, acetaminophen is safer than ibuprofen, provided you use it as directed. I think most doctors agree with this. In fact, I think many doctors think it’s obvious. (Source: I asked some doctors; they said it was obvious.)
Should this have been obvious to me? I figured it out by obsessively researching how those drugs work and making up a story about metabolic pathways and blood flow, and amino acid reserves. It’s a good story, one that revealed that my logic stemmed from an egregious lack of respect for biology and that I’m a big dummy (always a favorite subject). But if the clearest road to some piece of knowledge runs through metabolic pathways, then I don't think that knowledge counts as obvious.
So how is a normal person meant to figure it out? Why doesn't the fact that acetaminophen is typically safer than ibuprofen appear on drug labels or government websites or WebMD? Are normal people supposed to figure it out, or has society decided that this is the kind of thing best left illegible?
Note: You should not switch medications based on the uninformed ramblings of non-trustworthy pseudonymous internet people.
Jul Quanouai
How does ibuprofen work?
Ibuprofen inhibits the body’s production of the Cyclooxygenase (COX) enzyme. This in turn inhibits the formation of messenger molecules involved in inflammation, which leads to less physical inflammation and thus less pain.
The same story is true for almost all over-the-counter painkillers, which is why they’re almost all considered “non-steroidal anti-inflammatory drugs,” or NSAIDs. This includes ibuprofen, aspirin, naproxen (Aleve), and a long list of related drugs. But it does not include acetaminophen.
How does acetaminophen work?
Nobody knows!
Like ibuprofen, acetaminophen inhibits some COX enzymes. But it does so in a weird way that barely affects inflammation or messenger molecules, so it’s unclear if this matters for pain reduction.
In the brain, acetaminophen is metabolized into a mysterious chemical called AM404. This activates the cannabinoid receptors and increases endocannabinoid signaling, which seems to reduce the subjective experience of pain. AM404 also activates the capsaicin receptor, which is associated with burning sensations that you’d normally expect to increase pain, but maybe some desensitization thing happens downstream? And maybe acetaminophen also interacts with serotonin or nitric oxide or does other stuff? How this all comes together to reduce pain is still somewhat a scientific mystery.
Aside: When trying to understand painkillers, it’s natural to focus on chemistry and molecular biology. But the unknown physical origins of consciousness are always nearby, looming ominously.
What risks does ibuprofen have?
In an ideal world, the only thing ibuprofen would do is reduce inflammation in the part of your body that hurts. But that is not our world. When ibuprofen inhibits the COX enzymes, it does so throughout the body. And mostly, that is bad.
For one, ibuprofen reduces production of mucus in the stomach. That might sound okay or even good. But stomach mucus is important. You need it to shield the lining of your stomach from your extremely acidic gastric juice.1 Having less mucus can lead to gastrointestinal problems or even ulcers.
Ibuprofen also affects the heart. When ibuprofen inhibits the COX enzymes there, this in turn inhibits one chemical that prevents clotting and another that causes clotting. In balance, this seems to lead to more clotting, and an increased statistical risk of heart attacks 2 . If you’re healthy, the risk of a heart attack from an occasional low dose of ibuprofen is probably zero. But if you have heart issues and take medium to large doses regularly for as little as a few days, this might be a serious concern.
Ibuprofen also affects the kidneys. If you’re stressed, or cold, or dehydrated, or take stimulants, your body will constrict your blood vessels. That squeezes your kidneys’ intake tube, depriving them of blood. Your kidneys don’t like that, so they release signaling molecules to locally re-dilate the blood vessels.
Trouble is, when ibuprofen inhibits COX enzymes in the kidneys, it inhibits those signaling molecules. If everything is normal, that’s okay, because the kidneys wouldn’t try to use those molecules anyway. But if your body has clamped down on the blood vessels, then the kidneys don’t have the tool they use to keep blood flowing, meaning they don’t get as much blood as they want. This is bad.3
There are many other less common side effects, including allergies, respiratory reactions in asthmatics, induced meningitis, and suppressed ovulation. If you take a lot of ibuprofen, this could hurt your liver. But the major concerns seem to be the stomach, the heart, and the kidneys.
What risks does acetaminophen have?
Acetaminophen also inhibits some COX enzymes. But unlike ibuprofen, the effect is minimal outside the central nervous system. Thus, acetaminophen has little effect on stomach mucus, blood clots, or blood flow, and so presents almost none of the risks that ibuprofen does.
Even so, if you take too much acetaminophen at once, you could easily die.
How does this happen? Well, when acetaminophen is metabolized by the liver, it’s mostly broken down into harmless stuff. But a small fraction (5-15%) is broken down by the P450 system into an extremely toxic chemical called NAPQI.
Ordinarily this is fine; your body creates and neutralizes toxic stuff all the time. For example, if you drank 20 grams of formaldehyde, you’d likely die. But did you know that your body itself makes and processes ~50 grams of formaldehyde every day? When liver cells sense NAPQI, they immediately release glutathione, which binds to NAPQI and renders it harmless.
But there’s a problem. If you take too much acetaminophen at once, the pathways that break it down into harmless stuff get saturated, but the P450 system doesn’t get saturated. This means that not only is there more acetaminophen, but also that a much larger fraction of it is broken down into NAPQI. Soon your liver cells will run out of glutathione to neutralize it. Then, NAPQI will build up and bind to various proteins in the liver cells (especially in mitochondria) causing them to malfunction and/or commit suicide. This can cause total liver failure.
So you should never take more than the recommended dose of acetaminophen.4 If you do take too much, you should go to a hospital immediately. They will give you NAC, which will replenish your glutathione and neutralize the NAPQI. Your prospects are good as long as you get to the hospital within a few hours. 5 6
Acetaminophen has lots of other possible side effects, like skin issues and blood disorders. But these all seem to be quite rare.
What if you have liver issues?
The primary concern with acetaminophen is liver damage. So if you have liver disease, then surely you’d want to avoid acetaminophen and take ibuprofen instead, right?
Nope. It’s the opposite. Liver disease shifts the balance of risk in favor of acetaminophen.
With liver disease, it’s hard for blood to flow into the liver, meaning that blood tends to pool in the abdomen. To counter this, blood vessels elsewhere in the body contract. This includes blood vessels around the kidneys.
Remember the kidneys? Again, when blood vessels are constricted, the kidneys send out signaling molecules to locally re-dilate the blood vessels. But those signaling molecules are blocked by ibuprofen. So if you have liver disease, taking ibuprofen risks starving your kidneys of blood just like if you were dehydrated.
Meanwhile, people with moderate liver disease are usually still able to process acetaminophen without issue, as long as it’s in smaller amounts. So doctors usually tell patients with liver disease to avoid ibuprofen and take acetaminophen instead, just with a maximum of two grams per day instead of four.
(Obviously, if you have liver disease, then you should talk to a doctor, I beg you, for the love of god.)
What about other situations?
The main takeaway from all this is that the risks of both drugs emerge from the madhouse of complexity that is your body. Surely there are some situations where acetaminophen is more dangerous than ibuprofen?
I tried to capture the most common situations in this table:

It’s actually fairly hard to find situations where ibuprofen is safer than acetaminophen. Possibly this is true if you’re hungover, but I would be very careful, because you tend to be dehydrated when hungover, raising the risk of kidney damage. (It’s probably optimal, from a health perspective, to avoid taking recreational drugs at doses that leave you physically ill the next day.)
Aside from hangovers, the only situations I could find where ibuprofen might be safer than acetaminophen are if you’re taking certain anti-seizure or tuberculosis drugs or maybe if you have a certain enzyme deficiency (G6PDD).
So...
What have we learned so far?
1. The body is really complicated!
2. The main risk of acetaminophen is liver damage by creating too much NAPQI. Taking too much at once can easily kill you. However, as long as you don’t take too much at once and your liver isn’t depleted, then your liver will maintain NAPQI levels at zero and it will be completely fine. And there are very few other risks.
3. Meanwhile, ibuprofen poses a risk of gastrointestinal issues, heart attacks, or kidney damage. The risk varies based on lots of factors like whether you’ve eaten food, whether you’re dehydrated, your blood pressure, and your heart health.7
4. Therefore, acetaminophen is probably safer, provided you never take too much.8
I don’t want to be alarmist. If you’re healthy, the risk from taking an occasional dose of ibuprofen as directed is extremely low. Given that so many people find that ibuprofen is more effective for many kinds of pain, it’s totally reasonable to use it. I do so myself.
Still, it seems to be the case that in the vast majority of situations, acetaminophen is saf_er_. Personally, if I have pain, I first take acetaminophen, and then add ibuprofen if necessary. I’m pretty sure many experts think this is somewhere between “sensible” and “obvious.”
But if acetaminophen is safer, then why don’t official sources tell you that?9 I can get doctors to admit this off-the-record. I can find random comment threads with support from people who seem to know what they’re talking about. But why does this fact never appear on government websites or drug labels?
Let’s look at those drug labels
In the U.S., the Food and Drug Administration (FDA) creates10 a “drug facts” label for over-the-counter drugs.
Here’s what that looks like for ibuprofen:
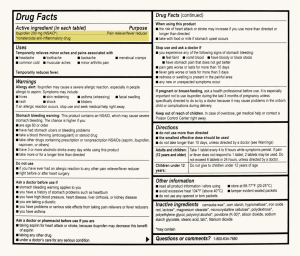
And here’s what it looks like for acetaminophen (acetaminophen):

I feel dumb saying this, but when I saw those labels in the past, I thought of them as a bunch of random information thrown together for legal reasons. But after spending a lot of time trying to understand these drugs myself, I now realize that these labels are... really good?
Imagine you work at the FDA and it’s your job to write a safety label. You need to synthesize a vast and murky scientific landscape. Your label will be read by people with minimal scientific background who are likely currently in pain, and who could die if they take the drug in the wrong situation.
If I were in that situation, I’d think about all the different situations in which taking one of these drugs could literally kill someone, and then — after a quick panic attack — I’d write a label that screamed, HEY, IF YOU ARE IN ANY OF THESE SITUATIONS, TAKING THIS DRUG COULD LITERALLY KILL YOU. Then I’d think about all the other situations where taking the drug might be okay depending on a set of complex science stuff and tell people in those situations to PLEASE TALK TO A DOCTOR FOR THE LOVE OF GOD because I DON’T KNOW IF YOU’VE HEARD BUT SCIENCE IS COMPLICATED. Everything else would be a minor concern.
From that perspective, these labels are a triumph. This isn’t random information — every word is a synthesis of a mountain of research, carefully optimized to save lives.
FDA good
How did those drug labels come to be?
If you want a taste for the FDA’s process, I encourage you to skim the 2002 Federal Register document in which the FDA proposed to update ibuprofen’s safety label and to formally classify it as Generally Recognized as Safe. It’s more than 21,000 words long and — I think — astonishingly good. It not only summarizes the entire medical literature on ibuprofen, it summarizes it well. Here is onerepresentative bit:
Bradley et al. (Ref. 42) conducted a 4-week, double-blind, randomized trial in 184 subjects comparing the effectiveness and safety of the maximum approved OTC daily dose of 1,200 mg of ibuprofen (number of subjects (n) = 62) to that of a prescription dose of 2,400 mg/day (n = 61), and to 4,000 mg/day of acetaminophen (n = 59) for the treatment of osteoarthritis. While there were no significant differences in the number of side effects reported during this study, the study demonstrated a trend towards a dose dependent increase in minor GI adverse events (nausea and dyspepsia) associated with higher doses of ibuprofen (1,200 mg/day: 7/62 or 11.3 percent; versus 2,400 mg/day: 14/61 or 23 percent). In addition, two subjects treated with 2,400 mg/day of ibuprofen became positive for occult blood while participating in the study.
I spend a lot of time complaining about bad statistical writing. A lot. Probably too much. But I’m here to tell you, that paragraph is gorgeous. The writing is clear and penetrating. It contains all the important details, but no other details. Compared to the abstract of the original paper, the above is shorter and easier to understand yet simultaneously more informative. Five stars.
The rest of the document is equally good, with clear and sensible explanations for various recommendations. For example, they discuss a proposal from the National Kidney Foundation for additional warning about risks to kidneys, explain why they think that proposal has merit, and then recommend a shorter version, which appears on every package of ibuprofen sold today.
As far as I can tell, this level of quality is typical. For example, the FDA’s 2019 proposed rule on sunscreens is similarly masterful.
So why?
This leaves us with this constellation of facts:
1. Acetaminophen is, in general, safer than ibuprofen.
2. The FDA doesn’t tell you that. Neither do other respectable authorities.
3. The FDA is highly competent.
So what’s happening here? Have the experts conspired to keep this knowledge secret?
I don’t think so. Mostly, I think this is down to two factors. First, the FDA doesn’t really have a mission of determining “in what circumstances is drug A safer than drug B?” Their goal is to take individual drugs and determine how people can use them safely. They seem to be quite good at this.
Second, everyone is mortally afraid of giving “medical advice.” It varies by jurisdiction, but in general, giving "wellness advice" is OK, but if you give personalized advice, you risk going to prison. The more credible you are, the higher that risk is.11
Stepping back, how should we think about this situation?
The body is complicated. When experts give the public advice on drugs, they are trying to insulate us from that complexity. But there is no way to do that without making trade-offs. Society has implicitly chosen tradeoffs that mean certain "less important" facts are de-prioritized. It’s not obvious that this is the wrong choice. I feel foolish for not having more respect for the body’s complexity and for the difficulty of the task all the experts are trying to accomplish. This is not medical advice.
- For some reason, humans have gastric acid that is more acidic than most other animals, and is only matched by animals that specialize in eating carrion.
- At least two NSAIDs (rofecoxib and valdecoxib) have been withdrawn from the market due to an increased risk of heart attacks. For the same reason, the US refuses to approve etoricoxib.
- Nephrologists hate ibuprofen. (Source: nephrologists.) If it was up to them, maybe ibuprofen would come with a “HAVE YOU CONSIDERED TAKING ACETAMINOPHEN INSTEAD?” warning. It confuses me that the safety label for ibuprofen doesn’t warn you about the danger of taking it while dehydrated and quietly damaging your kidneys. My best guess is that this is because other doctors don’t hate ibuprofen as much as nephrologists.
- Watch out for combination medicines (like cold or flu medicines or opiate painkillers) that include acetaminophen. Arguably, acetaminophen is a victim of its own success here. It’s included in these things because it is better tolerated than NSAIDs. But it’s easy to miss.
- Oddly, NAC is considered a nutritional supplement, meaning basically anyone can buy it. But there’s also almost no regulation, so who knows if the thing you bought actually has NAC in it? Do not screw around trying to self-medicate an acetaminophen overdose. Go to a hospital.
- At one point while researching all this I had what I thought was a good idea: Why not sell acetaminophen in pills bundled together with NAC? The NAC would replenish glutathione stores in the liver, seemingly reducing the risk of overdose. Later on, I developed more humility and felt very stupid for fantasizing that such an obvious idea could be novel or useful. I think that this is indeed a bad idea because NAC itself has side effects, though I can’t find much formal discussion. In fact, I found a 2010 editorial called "Why Not Formulate an Acetaminophen Tablet Containing N-Acetylcysteine to Prevent Poisoning?" In another study, Nakhaee et al. (2021) actually tried giving NAC together with acetaminophen to rats and found that this seemed to make it better at reducing pain. So maybe this isn’t a completely stupid idea. That last paper also led me to discover that “rat hot plate test” is a standard phrase, and one that drives home what humanity’s dominion over nature means in practice.
- Above, we mentioned that acetaminophen overdose is estimated to cause around 500 deaths per year in the U.S. It’s much harder to give direct numbers for how many people die from taking ibuprofen, because NSAIDs don’t really directly “kill” people, but rather increase the risk of dying in various ways. The best estimates seem to be that NSAIDs cause 5,000-16,500 deaths each year in the US via gastrointestinal complications, and something similar via heart attacks. These numbers are not a good way of quantifying the relative risk of drugs, because they represent different people taking different amounts for different reasons. But they do show that ibuprofen is not without risk.
- There are probably some people who are too disordered to track much acetaminophen they’ve taken. For such people, ibuprofen might be the safer choice. Though I’m skeptical that many such people are found among the readers of Asterisk.
- There are two cases where official sources are clear that acetaminophen is safer than ibuprofen: for use by pregnant women and small children. This doesn’t appear on the safety label, but if you’re pregnant and go to a doctor, they will probably tell you to take acetaminophen but not ibuprofen or other NSAIDs. And if you have a newborn baby, their doctor will probably tell you that you can give them acetaminophen but not ibuprofen or other NSAIDs.
- Technically, for many drugs today, it is the drug manufacturer that "creates" the label, which is why they can be slightly different. However, the FDA strongly regulates what is on it, including most of the language and even details about the font and so on. The federal register contains a template the FDA published for ibuprofen which is almost identical to what appears on the side of drugs today
- Unlike in most places, in the United Kingdom it seems to be perfectly legal for people to give each other medical advice, provided they don’t misrepresent themselves as licensed doctors. This is not legal advice.